
This appliance is a combination of several appliance designs with some small modifications. In fact it is a hybrid of the appliances of Dr Harold Gelb, Dr Brendan stack, etc. This appliance is designed to correct skeletal, muscular, tendon and ligament asymmetries. Therefore, it fulfils the criteria for an orthotic.
The purpose of orthotic therapy is to restore function and reduce symptoms, not to restore all of the injured or degenerative components back to their original dimensions and health. This appliance is produced on the mandible for aesthetics and function. If the patient cannot speak with the appliance in place, it is likely they will not wear the appliance
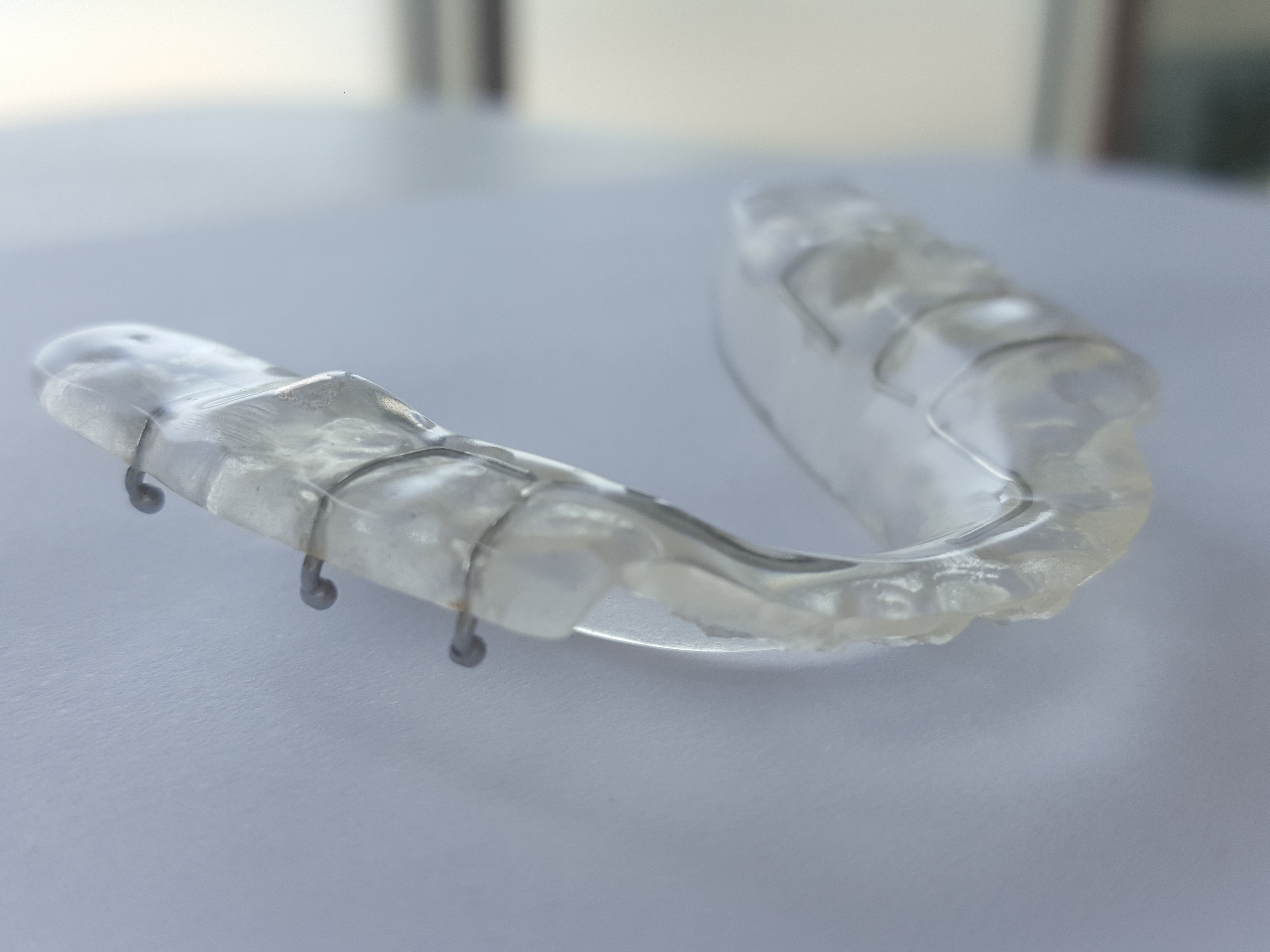
Design criteria of OD3 aims to provide more tongue space with the same ability occlusally as OD1/OD2 appliances. OD3 is basically an OD1 except for the use of thermoformed material as a substructure.
This appliance (OD3) is the most commonly prescribed day appliance for TMD therapy.
Wire braid strengthener can be added to the lingual area of OD3 appliances to provide more long term stability. Please note- Wire braid strengthener is not included in standard OD3 design as there is a slight intrusion on tongue space with this additional component. It requires coverage with acrylic which also leads to bulk in the tongue space. You must request this inclusion on our lab prescription forms.
Indications for Mandibular Day Positioned Orthotic
Chronic/acute dysfunction of intra-capsular origin (disc placement), TM joint inflammation (capsulitis), or skeletal and muscular asymmetry. It can also be used as a positioning stent to correct vertical dimension, rotational, cant and protrusive changes that have occurred due to attrition, restorations, or are of a developmental nature prior to prosthodontic rehabilitation.
The goal of this appliance is to provide the best condyle-fossa relationship possible at the time of treatment. Limitations as to positioning may be affected by capsular adhesions, skeletal fracture and previous surgery (orthognathic, TM joint reconstructive surgery). That does not mean that it is possible to recapture all displaced discs. In fact, there is no attempt to accomplish this.
The purpose of this appliance is to hold the position after the disc has been recaptured through either superior compartment injection or manual manipulation or the use of a pivot splint. Recapturing a displaced disc is more likely to happen when the displacement is early in translation. The later the reduction of the disc in opening, the less chance you have of recapturing by simply using an appliance.
Recapturing a displaced disc is based on the amount of ligament stretching that has occurred between the disc to condyle, disc to temporal bone, and condyle to temporal bone relationships. It may not be possible or it may be impractical to move the mandible to a position that recaptures the disc. In other words, it doesn’t make sense to place the patient who was originally in a Class I relationship and move them to a Class III relationship in order to recapture. They may have translated past the eminence at this point, which is obviously not a position that can be restored to, in needed. So again the goal is to create the proper spacing between condyle and fossa, then secondly to change the ligamentous relationships (undo the stretching, prolo therapy injections). If you want documentation as to the efficacy of condyle-fossa positioning as opposed to flat plane occlusal splint there is plenty.
The patient must be able to bite in reproducible, neuromuscularly comfortable and functional position. This is a mandibular acrylic appliance that covers the posterior occlusal surfaces and the lingual surfaces of the lower anteriors to within three mm of the incisal edges. This is necessary to prevent against extrusion or rotation of teeth during therapy. Covering the incisal edges dramatically effects speech but is sometimes necessary if the patient is posteriorly edentulous, either unilaterally or bilaterally. Centric stops provide the patient with reproducible occlusion. The mandibular anteriors can be covered with minimal distortion when using the OD1 appliance.
Indications for Mandibular Day Positioned Orthotic
Chronic/acute dysfunction of intra-capsular origin (disc placement), TM joint inflammation (capsulitis), or skeletal and muscular asymmetry. It can also be used as a positioning stent to correct vertical dimension, rotational, cant and protrusive changes that have occurred due to attrition, restorations, or are of a developmental nature prior to prosthodontic rehabilitation.
When your need to recapture a displaced disc.
READ PROFILE
Mandibular Orthopedic Re-positioning Appliance.
READ PROFILE
Minimally invasive design with wire major connector.
READ PROFILE
